100 Years of Respiratory Protection History (NIOSH)
In the News

In 1919, the U.S. Bureau of Mines (USBM) initiated the first respirator certification program. Several months later, on January 15, 1920, this federal body certified the first respirator. To recognize the important milestones of the past 100 years, this webpage documents a general historical overview of respiratory protection research and the evolution of the certification program as undertaken by the U.S. federal government.
Respiratory Protection History Prior to the 1800s
Around the world, scientific minds recognized the need for respiratory protection long before the U.S. Bureau of Mines. The history of respiratory protection traces back as far as Pliny the Elder (23-79 AD), a Roman philosopher and naturalist, who made use of loose animal bladder skins to filter dust from being inhaled while crushing cinnabar, which is a toxic, mercuric sulfide mineral used at the time for pigmentation in decorations. Many centuries later, Leonardo da Vinci (1452-1519) recommended the use of wet cloths over the mouth and nose as a form of protection against inhaling harmful agents (Spelce et al., “History,” 2018; Cohen and Birkner, 2012).
Further scientific inquiry and discovery led to the use of early atmosphere-supplying respirators. While ancient divers used hoses and tubes for supplied air, seventeenth century scientists added bellows to these devices as a way of providing positive pressure breathing. Although science has Pliny the Elder, photo courtesy of Shutterstock made advancements over time, the need for proper respiratory protection became increasingly apparent. In the 1700s, Bernadino Ramazzini, known as the father of occupational medicine, described the inadequacy of respiratory protection against the hazards of arsenic, gypsum, lime, tobacco, and silica (Spelce et al., “History,” 2018; Cohen and Birkner, 2012).
While these scientific discoveries and advancements to respiratory protection were pivotal, the most important date for respiratory protection was still to come.


1800s – 1920
Nealy Smoke Mask from The National Fireman’s Journal December 8, 1877
The 18th and 19th centuries achieved the development of what we would recognize today as respirators, far surpassing the use of animal bladders and wet cloths. In 1827, the Scottish botanist Robert Brown discovered the phenomenon known as the Brownian movement – the theory that collisions of rapidly moving gas molecules causes the random bouncing motion of extremely small particles. Understanding the behavior of small particles, the properties of filter media and their interactions led to the first particulate respirator. In the mid-1800s, German scientists conducted studies with industrial dust and bacteria and their relationship with respiratory health. In 1877, the English invented and patented the Nealy Smoke Mask. The Nealy Smoke Mask used a series of water-saturated sponges and a bag of water attached to a neck strap. The wearer could squeeze the bag of water to re-saturate the sponges to filter out some of the smoke. (Coffey, 2016; Cohen and Birkner, 2012; Kloos, 1963).
On July 1, 1910, the U.S. Department of the Interior established the United States Bureau of Mines (USBM). The USBM worked to address the high fatality rate of mineworkers. In 1919, the USBM initiated the first respirator certification program in the United States. In 1920, MSA Safety Company manufactured the Gibbs respirator. This closed-circuit self-contained breathing apparatus (SCBA) operated on compressed oxygen and a soda lime scrubber to remove carbon dioxide. (Spelce et al., 2017). According to MSA Safety Company, industries, fire departments, and health departments were the first to utilize the Gibbs Breathing Apparatus (WebApps.MSANet.com). The U.S. Navy requested a respirator comparable to those used for emergency escape purposes for mineworkers, leading to the invention of the Gibbs breathing apparatus, named for United States Bureau of Mines engineer and inventor W.E. Gibbs. Gibbs also created a respirator specifically for aviators (Spelce, et al., 2017).

World War I presented a new kind of threat to soldiers – chemical warfare gases, such as chlorine, phosgene, and mustard gas. The U.S. War Department asked the USBM to develop gas mask standards. Military equipment at the time did not account for protective masks or respirators. Combat equipment did not include respirators until World War II (Caretti, 2018). As a result, chemical warfare in WWI accounted for 1.3 million casualties and approximately 90,000 fatalities. This amounted to about 30% of all casualties during the war (Fitzgerald, 2008).
Additionally, WWI troops from all over the world helped a new influenza virus spread. The lack of vaccines and respiratory protection contributed to high fatalities from the flu virus. The U.S. reported the first flu symptoms in March 1918. In October of 1918 alone, the flu virus killed 195,000 Americans resulting in the San Francisco Board of Health recommending the use of masks in public spaces. The pandemic flu began to decline in early 1919. The flu caused approximately 50 million deaths across the world, including 675,000 in the United States (“1918 Pandemic,” 2018). The spread of the pandemic flu at this time displayed the need of additional respiratory protection and research needed in healthcare settings.
While the flu pandemic exhibited a need for healthcare respiratory protection, researchers at the time still largely focused on the respiratory protection of mining. On March 5, 1919, the USBM produced Schedule 13, “Procedure for Establishing a List of Permissible Self-Contained Oxygen Breathing Apparatus.” Schedule 13 set the first set of regulations for human testing of protection of self-contained breath apparatus respirators and certification thereof (Kyriazi, 1999). Finally, on January 15, 1920 the USBM certified the first respirator, the Gibbs breathing apparatus. (Spelce et al., “History,” 2018; Cohen and Birkner, 2012). The Gibbs breathing apparatus, originally designed for mine work, became the first approved respirator for industrial work. (Spelce, et al., 2017).

1920 – 1950
Gibb’s Breathing Apparatus
During World War I, the U.S. government sought improvements for respiratory protection across several industries as well as the military. The passing of the Overman Act of May 20, 1918 by President Wilson gave authority for the Army to lead the research efforts in respiratory protection in order to engage in chemical warfare and defense. However, this delegation of research power was short-lived, and the USBM regained the primary task of mine safety research. (Spelce, et al., 2017).
The USBM developed Schedule 14 shortly after for the certification of military-use gas masks. Over time, the USBM altered Schedule 14, “Procedure for Establishing a List of Permissible Gas Masks,” several times. Initial modifications to it included acknowledgement of the 1941 USBM “Facepiece Tightness Test” which tested the detectable leakages and freedom of movement of the user (Spelce, et al., “History” (Cont.), 2018).
Because of the horrific casualties of WWI from chemical warfare, armed forces on both sides of the battlefield refrained from using chemical agents during WWII. Both sides shared the paranoia that the enemy had more harmful chemical warfare agents (Chauhan, 2008). As the world entered World War II, the U.S. Navy’s use of asbestos increased for insulation purposes for pipes in naval vessels. It was not until 1939 that a Medical Officer for the U.S. Navy recognized the need for crew to wear respirators when cutting and wetting amosite and other asbestos containing insulation. Later, as the U.S. entered World War II, Fleischer et al. released a study acknowledging the dangers and risks of dust exposures in asbestos insulation manufacturing. However, even after the publication of the Fleischer et al. study in 1946, the U.S. Navy continued to use asbestos with the additional warning that “exposure to asbestos dust is a hazard which cannot be overlooked in maintaining an effective occupational-hygiene program.” The Navy continued to recommend confinement of pipe covering operations, and the use of respirators and ventilation (Barlow et al., 2017).
In the early 1930s, the Hawk’s Nest Tunnel disaster occurred in West Virginia. The estimated death toll, one of the worst in American industrial history, ranges from roughly 700-1,000 deaths of the 3,000 who worked underground. The tragedy of this disaster expedited the publication of the USBM’s first approval of dust/fume/mist respirator approval standards in 30 CFR Part 14, Schedule 21 (USBM 1934). “The USBM had already developed standards for and approved oxygen breathing apparatus (1919), gas mask respirators (1919), and hose mask respirators (1927). By 1937, the Bureau expanded its schedule for testing hose masks to include a variety of supplied-air respirators including Type CE abrasive blasting respirator” (Spelce, et al., 2019). Schedule 21 describes several types of respirators, including Type A, B, C, combinations of A-C, and D (Spelce, et al., 2019). The original Schedule 21 from 1934 included the following requirements:
- Exhalation valves were required, and inhalation valves were optional
- Added Pressure-Tightness Tests to assess the fitting characteristics of the respirator
- Revised the Direct Leakage and Man Test (coal dust test) by eliminating work exercises
- The high concentration silica dust defined the test period as one 90-minute test, not three 30-minute test periods
- Eliminated the low concentration Silica Dust Test
- Water Silica Mist and Chromic Acid Mist Tests defined the sampling period after 156 minutes and after 312 minutes, respectively
- Added a Lead Dust Test
- Eliminated the Lead Paint Test
Revisions to Schedule 21 expanded in 1955 under 30 CFR 14 to include the approval respirators with single use filters and reusable filters. Among these, there are two classes of respirators, including approval for protection against Pneumoconiosis and approval against dust that were not more toxic than lead. These approvals expanded to also included protection against lead fumes, silica, and chromic acid mists (Spelce, et al., 2019).
The USBM began to set stricter regulations on respirators during WWII. It established “certain basic requirements applicable to all types of respiratory equipment. These requirements are as follows: (1) They must give adequate protection; (2) they must be reasonably comfortable and physically convenient to wear; (3) they must provide an acceptable period of protection; and (4) they must be constructed of durable materials. (IC 7130, August 1940, page 5)” (Spelce et al., 2018; D’Alessandro, 2018). The regulation of respiratory protection permitted the standardization of higher quality respiratory protection.
After WWII and the use of chemical gas in warfare, researchers continued their work on improving respiratory protection for soldiers. The events of World War II and the boom of industry on the home front exhibited a need for improved respiratory protection in industry. Americans on the home front went to work on the production lines to aid the war effort, ushering in a booming era of industry and manufacturing. However, those workers inhaled high amounts of asbestos due to poorly regulated working conditions. Early accounts from turn of the century industrial hygienists documented the dangers of airborne asbestos in working environments, but it was not until the mid-1950s that prolonged exposure to asbestos caused widespread concern. Research efforts still did not fully serve this need until even later, in the 1960s and 1970s. “With the introduction of the membrane filter sampling method in the late 1960s and early 1970s, asbestos sampling and exposure assessment capabilities advanced to a degree which allowed industrial hygienists to more precisely characterize the exposure–response relationship” (Barlow et al., 2017).
Researchers performed tests on respirators to measure protection, but their levels of protection were unregulated. There was not yet a system in place to set a threshold standard of protection nor any regulatory body in the manufacturing of respirators. The respirators used in different settings, such as in construction or commercial farming, lacked regulation to ensure necessary protection against the airborne hazards in these types of settings.
Further, Schedule 21B in 1965 expanded. These changes include (1) extend certification of approval to respirators designed to protect against dusts, fumes, and mists that are significantly more toxic than lead; (2) permit certification of combinations of dispersoid-filter and other types of respirators; (3) revise current tests to realize accuracy and speed of testing; and (4) revise the fees for inspection and testing (USBM, 1964) (Spelce, et al., 2019). This provided further regulation and protection for industrial workers’ respiratory health.
“The use of respirators continued unregulated until the Federal Coal Mine Health and Safety Act was enacted in 1969, resulting in regulations governing the certification and use of respirators in the mining industry. The Occupational Safety and Health Act, which established the Occupational Safety and Health Administration (OSHA) and the National Institute of Occupational Safety and Health (NIOSH), was promulgated in 1970” (Cohen and Birkner, 2012).
According to the Occupational Safety and Health Act of 1970, “The Congress finds that personal injuries and illnesses arising out of work situations impose a substantial burden upon, and are a hindrance to, interstate commerce in terms of lost production, wage loss, medical expenses, and disability compensation payments” (91st Congress, 1970). Further, the OSH Act of 1970 acknowledges a need for regulation in the safety and health of working citizens to preserve “human resources.” The document sets standards for work places to maintain as well as formulate a regulatory body to oversee the adherence to these standards. The OSH Act not only sets standards to protect workers from physical injury and disease, but also acknowledges the necessity to protect workers from psychological harm in the workplace, such as anxiety linked to physical injury risk at work.
The OSH Act also established the National Institute for Occupational Safety and Health (NIOSH) as a research body focused on the health, safety, and empowerment of workers to create safe and healthy workplaces (NIOSH, “About”). OSHA and NIOSH continue to be important organizations that assist in safety recommendation and regulation in the workplace, in the area of respiratory protection as well as other areas of personal protective equipment.
1970 – 2000
“Congress created the Occupational Safety and Health Administration (OSHA) in 1970, and gave it the responsibility for promulgating standards to protect the health and safety of American workers. On February 9, 1979, 29 CFR 1910.134 gained recognition as applicable to the construction industry (44 FR 8577). Until the adoption of these standards by OSHA, most guidance on respiratory protective devices use in hazardous environments was advisory rather than mandatory” (Department of Labor, 1998). OSHA reprinted, without change of text, 29 CFR Part 1926 with the General Industry Occupational Safety and Health Standards in 29 CFR part 1910. This has since become a set of OSHA regulations (“Editorial Note,” 1978).
In 1994, the U.S. Centers for Disease Control and Prevention (CDC) released a Morbidity and Mortality Weekly Report entitled “Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Facilities, 1994.” This document revises the 1990 tuberculosis (TB) guidelines in response to an outbreak in 1991 and studies from 1985 that show a multi-drug resistance to the bacterium that causes TB. These guidelines emphasize importance of healthcare professionals’ proper use of personal protective equipment (PPE), specifically respiratory protection. Areas of emphasis for respiratory protection include ventilation, donning, use, and doffing. Finally, the guidelines address the need to maintain a full respiratory protection program within healthcare settings, ensuring all healthcare workers train in proper PPE use. This is of particular importance for healthcare workers that move from department to department, such as therapists, dieticians, maintenance, interns, etc.
As respiratory protection became mandatory, the importance of a tight and proper respirator fit increased. In 1995, OSHA revised the certification regulations for fit testing. This led to further research in 1996 regarding exposure in the workplace, causing researchers to use simulated workplace protection factors and exposure simulations (Cohen and Birkner, 2012; Department of Labor, 1998).
“On 10 July 1995, the respirator certification regulation, 30 CFR 11, was replaced by 42 CFR 84 (NIOSH, 1995). The primary regulatory changes introduced by 42 CFR 84 are associated with a new approval concept, performance requirements for particulate respirator filters, and instrumentation technology. 42 CFR 84 updated filter requirements and tests to provide an assessment of the effectiveness of the filter based upon its efficiency to remove particulates of the most penetrating size from the ambient air regardless of the particulate composition and toxicity (NIOSH, 1994). The approval philosophy for filters changed from minimum requirements considered safe to breathe for various types of dust/fume/mist respirators to acceptable filter efficiency levels against laboratory generated aerosols with particles of the most penetrating size” (Spelce, et al., 2019).
The OSHA respiratory protection standard, 29 CFR 1910.134, published on January 8, 1998, replaced the agency’s original standard promulgated in 1972. The rule standardized regulations for respirator use in all industries, including maritime, construction, and general industry. However, this did not include updates for the respiratory protection of the healthcare industry, which at this time still functioned under 29 CFR 1910.134 regulations. While this new development did not include the use of respirators in the healthcare setting, it did effectively progress industry, manufacturing, and construction towards a more healthy and safe work environment.
The necessity for respiratory protection in the healthcare setting came to the forefront of concern with the outbreak of tuberculosis in the 1990s. According to the TB Respiratory Protection Program in Health Care Facilities: Administrator’s Guide, “The use of respirators in the health care setting is a relatively new but important step forward in the efforts to prevent the transmission of tuberculosis (TB). Air-purifying respirators provide a barrier to prevent health care workers from inhaling Mycobacterium tuberculosis. The level of protection a respirator provides is determined by the efficiency of the filter material and how well the facepiece fits or seals to the health care worker’s face. A number of studies have shown that surgical masks will not provide adequate protection in filtering out the TB organism. Additionally, surgical masks are not respirators and therefore, are not NIOSH-certified and do not satisfy OSHA requirements for respiratory protection”(1999).

2000 – 2019
In 2001, Congress requested the creation of a division within NIOSH to focus on the improvement and research of PPE and personal protective technologies (PPT). This division, the National Personal Protective Technology Laboratory (NPPTL) conducts scientific research, develops guidance and authoritative recommendations, disseminates information, and responds to requests for workplace health hazard evaluations.
The focus for respiratory protection research shifted drastically in the early 2000s when national tragedy struck. On September 11, 2001, terrorist attacks in New York City, Shanksville, PA, and Washington D.C. led to first responders in these cities, as well as nationally, to jump into action. The employees of NIOSH NPPTL also mobilized. According to NIOSH NPPTL employee Robert Stein, “If anyone ever doubted the potential for impact on a vast scale, those doubts should have been firmly dispelled the morning of September 11, 2001. I was sitting at my desk that was in building 02 at the time when I got a phone call from one of my colleagues who was off site that day. He said, “They are flying planes into the World Trade Center.” I had already heard the news that an airplane had hit one of the World Trade Center towers, but his was the first voice to identify and call it out as an intentional act. Things started to develop rapidly after that. The personnel at the newly formed lab gathered to develop response plans. Response planning quickly evolved into planning for communication contingencies as we got word that government sites would be evacuated. Obedient to the directions to leave the work site, several of us mustered at the nearby home of one of our colleagues to finish up with our what-if’s and how-to-get-in-touch-with’s. It was an eerie ride home, very confusing to the senses travelling under the beautiful blue skies of a perfect late summer day, but with such serious and unknown threats seemingly looming everywhere.
Even while there was still a ban on commercial flights, NPPTL sent two individuals to the World Trade Center site to help with respiratory protection issues as they were occurring. Not only were they able to provide immediate assistance at the World Trade Center site, but the first-hand experience they gained observing the difficulties encountered trying to provide respiratory protection to such a large number of first responders, recovery workers, law enforcement personnel, and other workers involved in the response helped to shape technical and policy decisions for months and years afterwards. The entire lab dedicated long hours in order to complete new statements of standard for respirator types with protections appropriate to protect first-responders involved in terrorist incidents, and then approve respirators so those new standards would actually result in providing appropriate respiratory protection for those workers.”
Following the terrorist attacks on September 11, 2001, the PPE used by first responders became a top priority for NIOSH, as it emphasized the PPE needed to protect those risking their own lives in order to save lives. In the weeks after September 11, the New York City Fire Department’s Bureau of Health Services (FDNY-BHS) and NIOSH launched a collaborative study. This study researched the effectiveness of personal protective equipment, including respiratory protection, and the occupational hazards and exposures of these first responders. The results indicated that many firefighters did not use adequate respiratory protection during the first week of the rescue/recovery operation (MMWR, 2002).
A study researched seven first responders to the attacks in New York on September 11 and their exposure to the dust at Ground Zero on September 11 or September 12. All were non-smokers or had only smoked in their distant past. The results of the study showed that all seven first responders developed some form of lung disease after their exposure to the dust at Ground Zero (Wu, et al., 2010).
Research suggests the rate of respiratory illness was so high due to a lack in use of respiratory protection. According to firsthand accounts by P.J. Lioy and M. Gochfeld in their 2002 article “Lessons Learned on Environmental, Occupational, and Residential Exposures from the Attack on the World Trade Center,” an alarmingly low number of individuals were using respiratory protection in the field at Ground Zero, and many that had respiratory protection were not wearing it (Crane et al., 2012).
The work to improve respiratory protection and subsequent guidance on use of respiratory protection has continued well after 2001. In 2005, NIOSH released its “Interim Guidance on the Use of Chemical, Biological, Radiological, and Nuclear (CBRN) Full Facepiece, Air-Purifying Respirators/Gas Masks Certified under 42 CFR Part 84.” According to NIOSH NPPTL employee, Jeff Peterson, “I would certainly say that one of the biggest accomplishments in the field of respiratory protection is the development of the voluntary NIOSH CBRN requirements.”
The CBRN requirements answered the need of emergency responders to maintain knowledge of PPE in a time of increased global terrorism. This interim guidance document provided guidelines for the selection and use of NIOSH-approved full facepiece, tight fitting, non-powered, air-purifying respirators (APR) for protection against quantified CBRN agents.
Following September of 2001, NIOSH and The RAND Corporation developed multiple volume reports dedicated to protecting emergency responders (Szalajda, 2008). NIOSH also developed three CBRN standards. The first requires that self-contained breathing apparatus (SCBA) meet CBRN protection standards because it “is used where the respiratory threat level is unknown or known to be immediately dangerous to life and health (IDLH)” (Szalajda, 2008).
Secondly, NIOSH developed a standard for a full-facepiece, air-purifying respirator. “The CBRN APR full-facepiece respirator is widely used by multiple responder groups. It provides a lower level of protection than the SCBA and its use is generally allowed once conditions are understood and exposures are determined to be at levels below those considered to be IDLH” (Szalajda, 2008).
The third priority was that air-purifying and self-contained escape respirators meet CBRN standards. This enabled a more general workforce, rather than those solely focused on first responders, to use PPE safely in a CBRN terrorist incident. As addressed by Deputy Director Jon Szalajda, NIOSH NPPTL “continues to develop criteria for additional types of respirators in response to responders’ needs for appropriate respiratory protection against the anticipated hazards faced in performing rescue and recovery operations resulting from viable terrorist threats, as well as HAZMAT incidents” (Szalajda, 2008).
In 2015, the American National Standard Institute (ANSI) standard Z88.2 updated the standard practice for respiratory protection. The Z88 Committee established the standard in 1969, with revisions in 1989 and 1992. The Z88.2 standard “sets forth minimally accepted practices for occupational respirator use; provides information and guidance on the proper selection, use and maintenance of respirators, and contains requirements for establishing, implementing and evaluating respirator programs. The standard covers the use of respirators to protect persons against the inhalation of harmful air contaminants and against oxygen-deficient atmospheres in the workplace” (ANZ88.2-2015, 1.1).
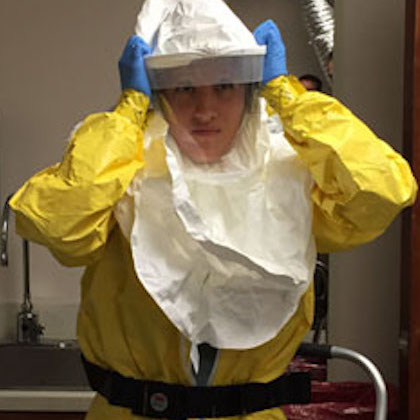
From 2014-2016, a global epidemic of the Ebola virus disease spread to the United States. During this time, proper PPE use in healthcare settings became a paramount concern, as the highly contagious virus spreads from contact with blood and other bodily fluids. Because of the virus’ highly contagious nature, the CDC recommended the use of a NIOSH-approved N95 respirator, or higher level of particulate filtration, or a powered air-purifying (PAPR) when caring for a Person Under Investigation (PUI) for the Ebola virus disease or a person with a confirmed case of the virus. Further, the CDC released guidelines for the disposal, cleaning, and disinfection based on the type of respirator worn by a healthcare worker when treating an Ebola patient. (Frequently Asked Questions, Ebola, 2018).
In 2019, “NIOSH NPPTL continues to provide national and world leadership in respirator approval, research, and standards development to support the workers who rely on respiratory protection,” states NPPTL Director, Dr. Maryann D’Alessandro. Such research includes understanding respirator comfort, fit, and usability; stockpiling of respirators; and rapid respiratory protection training in healthcare settings.
One hundred years have passed since the first approved respirator. NPPTL continues to provide respiratory protection research to best serve the workers and public that relies on them.